Preparing for this Test
Important Considerations Before Testing
Certain medications and supplements may impact test results, though in some instances that impact is unknown. There are many substances that influence cortisol and DHEA levels, however no known substances will interfere with the ability to run the assay itself.
Genova never recommends that patients discontinue medically necessary medications or supplements in order to complete testing.
There may be times when a patient may stay on a medication or dietary supplement during testing in order to evaluate its effectiveness or impact. A clinician may choose to discontinue a substance in order to evaluate the patient's baseline. The timeframe to discontinue varies for each substance and is at the discretion of the clinician.
Any questions regarding a medication or supplement impact on biomarker results can be researched by contacting the medication/supplement manufacturer and/or searching the literature (PubMed, Google Scholar) for relevant information. Drug databases such as drugs.com, rxlist.com, or Epocrates may provide additional information.
Glucocorticoids
Any steroid-based preparation including oral, topical (patch, cream), eye drops (minimal impact), nasal sprays, injections, and inhalers may influence the Adrenal Stress Profile findings.1-11 The degree of impact depends on numerous factors including, but not limited to, preparation, specific drug, dosage, chronicity of use, and individual response to medications. Not all glucocorticoids impact results the same.7
In general, exogenous glucocorticoids - even with one-time administration - are known to suppress the HPA axis via negative feedback, which can result in lower endogenous production of cortisol.3,12,13 Long-term use of glucocorticoids can lead to adrenal atrophy, which is slowly reversible.12,13 Glucocorticoid-induced adrenal insufficiency may last up to 2-4 years after glucocorticoid withdrawal.14
When to test a patient following glucocorticoid discontinuation is dependent on multiple factors (mentioned above) and is at the discretion of the clinician. For example, if a clinician wishes to test a patient's baseline HPA axis function following a steroid injection, it may take up to 4 weeks or longer for recovery to baseline.6,8 A literature search may provide further insight into the clearance rate and impact the particular glucocorticoid may have on salivary testing.
The cortisol assay can cross-react with various glucocorticoid drugs. For example, there is a strong cross-reactivity with the antibody used in this assay and dexamethasone which may result in a false elevation of cortisol. It is unknown how much of the reported result is the patient's endogenous cortisol, versus how much is cross-reactivity from the medication.
Genova's hormone assays measure endogenous hormones as well as bioidentical hormone replacement, but not synthetic hormones, due to their different molecular structure. Hydrocortisone is bioidentical cortisol and is prescribed for patients with adrenal insufficiency. Some studies suggest utility of salivary cortisol measurements for monitoring glucocorticoid replacement therapy, however studies are mixed.15
Shift Workers and Alternate Sleep-Wake Schedules
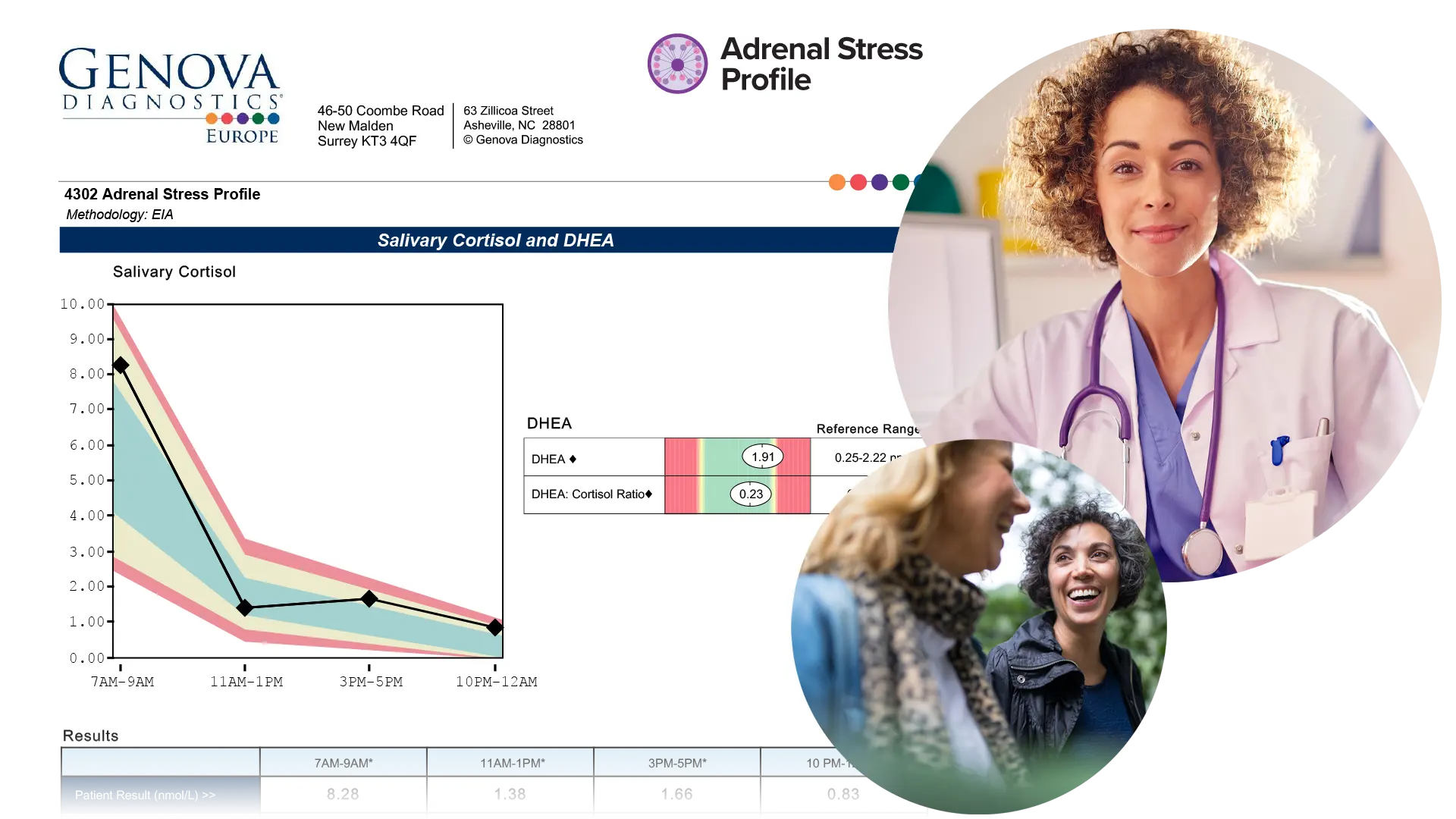
The reference ranges for the Adrenal Stress Profile (ASP) were designed for patients with normal sleep cycles and referenced for the specific time frames as graphed on the test report. However, some clinicians choose to test individuals with altered sleep cycles, knowing that the graph, and reference ranges may not directly apply. Even though the reference ranges may not apply, there is still some clinical information to be gleaned based on the overall slope of the diurnal curve. It is unknown whether extrapolating from the diurnal curve and reference ranges would apply to someone on an alternate schedule - "healthy" or "normal" has not been defined for this population.16-19 If the clinician chooses to test, the clinician can change the morning peak time to the patient's waking time (within one hour of waking) and then each additional sample will be approximately four hours after the prior.
In order to determine cortisol awakening response (CAR), samples must include both the waking and 30-minute samples. The timing of these collections should reflect when the patient wakes to begin their day. It has been shown in literature that patients who have alternate work schedules may 'reset' their internal circadian rhythm and, therefore, CAR sampling can be done during their normal waking cycle. When the patient wakes, have them immediately give a saliva sample, then another exactly 30 minutes later for CAR. These two samples are used for the CAR calculation. The third sample should be within that hour, then every four hours after that to complete the ASP portion.
Bleeding Gums
Samples visibly contaminated with blood should be recollected. This can result in a false elevation of hormones. Blood concentrations of steroid hormones are several-fold higher than saliva levels.20,21 For this reason, brushing and flossing is discouraged for 1 hour prior to salivary collection. Additionally, if the patient has a condition that causes gums to bleed easily, such as gingivitis or periodontitis, or has dentures and other oral appliances, a plan should be in place to ensure gums do not bleed during testing.
Paediatric Patients
The reference ranges for the Adrenal Stress Profile are based off a healthy cohort of patients aged greater than 18. Genova does not have pediatric reference ranges. DHEA is an androgen and is typically lower in prepubescent populations. A literature search may provide further insight into pediatric reference ranges for cortisol and DHEA.
REFERENCES
- Pandya D, Puttanna A, Balagopal V. Systemic effects of inhaled corticosteroids: an overview. The Open Resp Med J. 2014;8:59-65.
- Sastre J, Mosges R. Local and systemic safety of intranasal corticosteroids. J Invest Allergol Clin Immunol. 2012;22(1):1-12.
- Baptist AP, Reddy RC. Inhaled corticosteroids for asthma: are they all the same? J Clin Pharm Therap. 2009;34(1):1-12.
- Stout A, Friedly J, Standaert CJ. Systemic Absorption and Side Effects of Locally Injected Glucocorticoids. PM & R : J Injury Function Rehab. 2019;11(4):409-419.
- Masharani U, Shiboski S, Eisner MD, et al. Impact of exogenous glucocorticoid use on salivary cortisol measurements among adults with asthma and rhinitis. Psychoneuroendocrinology. 2005;30(8):744-752.
- Habib GS. Systemic effects of intra-articular corticosteroids. Clinical Rheumatol. 2009;28(7):749-756.
- Broersen LH, Pereira AM, Jørgensen JO, Dekkers OM. Adrenal Insufficiency in Corticosteroids Use: Systematic Review and Meta-Analysis. J Clin Endocrinol Metab. 2015;100(6):2171-2180.
- Chon JY, Moon HS. Salivary cortisol concentration changes after epidural steroid injection. Pain Phys. 2012;15(6):461-466.
- Silver S, Tuppal R, Gupta AK, et al. Effect of calcipotriene plus betamethasone dipropionate topical suspension on the hypothalamic-pituitary-adrenal axis and calcium homeostasis in subjects with extensive psoriasis vulgaris: an open, non-controlled, 8-week trial. J Drugs Dermatol. 2013;12(8):882-887.
- Krupin T, Mandell AI, Podos SM, Becker B. Topical corticosteroid therapy and pituitary-adrenal function. Arch Ophthal. 1976;94(6):919-920.
- Sandhu SS, Smith JM, Doherty M, James A, Figueiredo FC. Do topical ophthalmic corticosteroids suppress the hypothalmic-pituitary-adrenal axis in post-penetrating keratoplasty patients? Eye. 2012;26(5):699-702.
- Ambrogio AG, Pecori Giraldi F, Cavagnini F. Drugs and HPA axis. Pituitary. 2008;11(2):219-229.
- Lipworth BJ. Systemic adverse effects of inhaled corticosteroid therapy: A systematic review and meta-analysis. Arch Int Med. 1999;159(9):941-955.
- Pelewicz K, MiÅkiewicz P. Glucocorticoid Withdrawal-An Overview on When and How to Diagnose Adrenal Insufficiency in Clinical Practice. Diagnostics. 2021;11(4).
- Jung C, Greco S, Nguyen HH, et al. Plasma, salivary and urinary cortisol levels following physiological and stress doses of hydrocortisone in normal volunteers. BMC Endo Dis. 2014;14:91.
- Cannizzaro E, Cirrincione L, Mazzucco W, et al. Night-Time Shift Work and Related Stress Responses: A Study on Security Guards. Int J Environ Res Public Health. 2020;17(2).
- Lindholm H, Ahlberg J, Sinisalo J, et al. Morning cortisol levels and perceived stress in irregular shift workers compared with regular daytime workers. Sleep Dis. 2012;2012:789274.
- Li J, Bidlingmaier M, Petru R, Pedrosa Gil F, Loerbroks A, Angerer P. Impact of shift work on the diurnal cortisol rhythm: a one-year longitudinal study in junior physicians. J Occup Med Toxicol. 2018;13:23.
- Bostock S, Steptoe A. Influences of early shift work on the diurnal cortisol rhythm, mood and sleep: within-subject variation in male airline pilots. Psychoneuroendocrinology. 2013;38(4):533-541.
- Hofman LF. Human saliva as a diagnostic specimen. J Nutr. 2001;131(5):1621s-1625s.
- Granger DA, Taylor MK. Salivary bioscience: foundations of interdisciplinary saliva research and applications. Springer Nature; 2020.